

Scenario
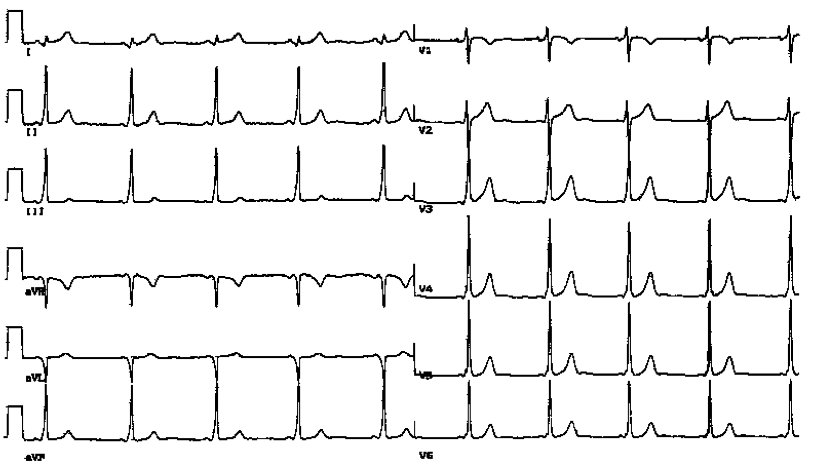
32-year-old man presented with cough, breathlessness on exertion and interscapular pain. His ECG was as below.
- Reassure
- CXR, reassure
- CXR, take a more detailed history, then reassure
- CXR, full history, refer for further assessment
Discussion
The patient has Wolff-Parkinson-White ECG with pre-excitation manifested by delta waves and a shortened PR interval. His main symptoms are likely a minor respiratory illness, hence making the ECG findings incidental.
A detailed history needs to be taken to ascertain family history of sudden cardiac death and personal history of palpitations, dizziness/faints or longstanding breathlessness on exertion. Occupational history (e.g. pilot, or heavy machinery operator) is also important.
WPW risk lies in rapidly conducted pre-excited SVT or AF, which may lead to hemodynamic compromise, VT, VF or even sudden death.
Investigations include
- Exercise tolerance test to assess the maximum rate of antegrade accessory pathway conduction. This is demonstrated by the disappearance of delta waves during exercise. If delta waves disappear at low heart rate, antegrade accessory pathway becomes refractory at a lower heart rate, conducts less rapidly, and hence less risky.
- Echocardiography to exclude structural cardiac abnormalities such as Ebstein’s anomaly and hypertrophic cardiomyopathy
- Holter monitoring if symptoms of palpitations
Treatment
- Radiofrequency ablation is successful in over 95% cases and is the mainstay of therapy.
- Acute pre-excited SVT cannot be treated with AV blocking agents such as betablockers, diltiazem and verapamil.
- Acute pre-excited SVT can be managed with procainamide (class I antiarrhythmic) or amiodarone (class III antiarrhythmic). Flecianide may also be considered.
Author
Dr Seif El-Jack