
GLP-1 Agonists - Frequently Asked Questions
What are these medications?
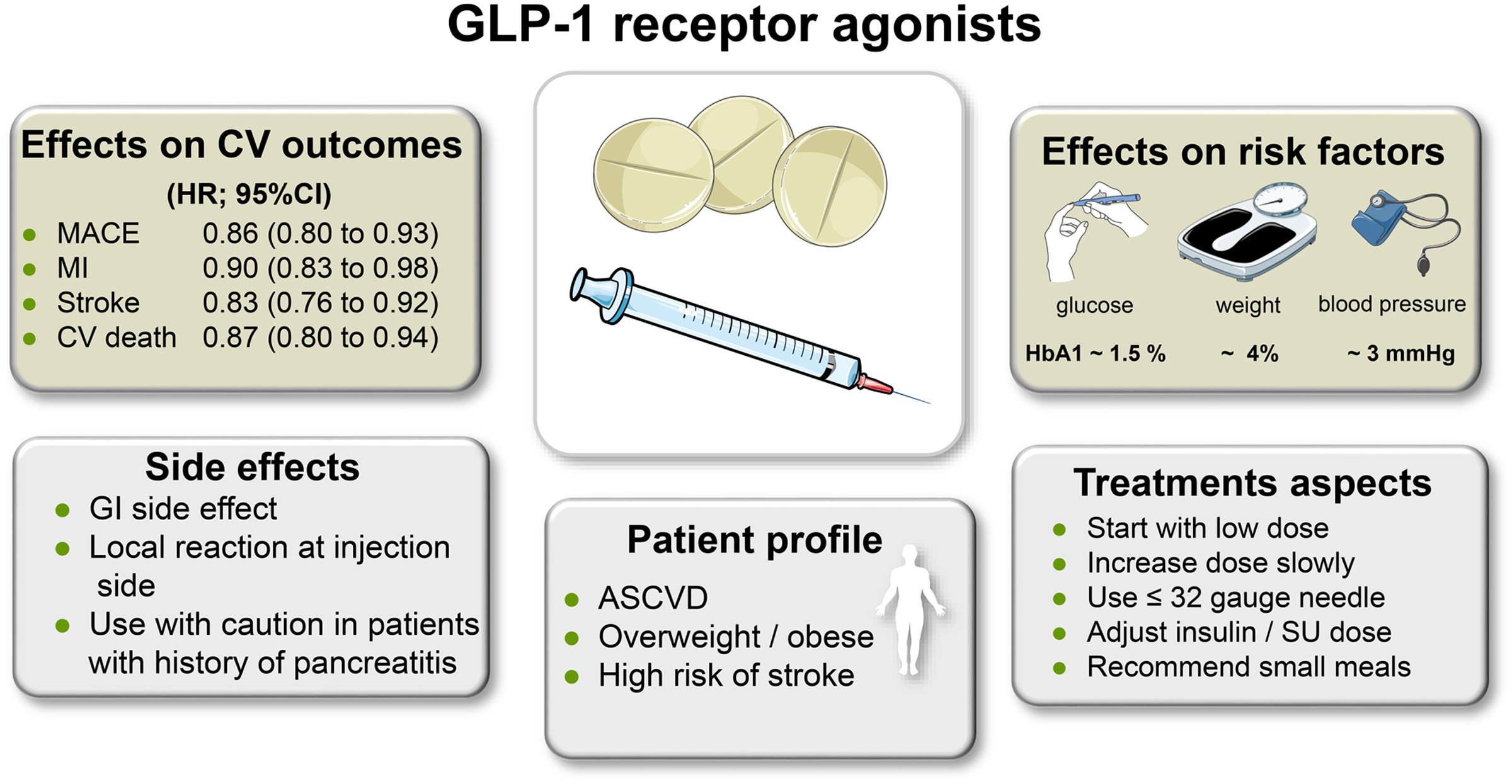
GLP-1 agonist is a class of medications that are used in type 2 diabetes and obesity.
Via the incretin pathway, they stimulate insulin release, suppress glucagon release, slow down gastric emptying, and enhance central satiety signal.
They, therefore, have favourable effect on glucose metabolism and lead to significant caloric intake reduction and resultant weight reduction, usually in the vicinity of 3 - 8 kg depending on the dose and agent used.
GLP-1 agonists are one of a few classes of diabetes medications proven to have cardiovascular, renal and mortality benefit in large-scale prospective randomised controlled trials.
They include Dulaglutide (Trulicity) and Liraglutide (Victoza / Saxenda).
Who are these for?
Diabetes - GLP-1 agonists should be primarily considered in patients with type 2 diabetes with suboptimal glycaemic control despite maximal tolerated dose of metformin (+/- other agents) especially where weight loss is desired and/or significant stroke risk is present.
Weight loss - GLP-1 agonists could also be considered for weight loss even in the absence of type 2 diabetes. Suggested cut-off is BMI >30, or >27 with weight related co-morbidity.
How to start?
Injection technique is relatively straightforward, similar to insulin; hence, GLP-1 agonists could be started in primary or secondary care.
Diabetes (Type 2)
Available in NZ = Dulaglutide (Trulicity, weekly injection) or Liraglutide (Victoza, daily injection).
Identical Pharmacy eligibility criteria to SGLT-2 inhibitor Empagliflozin, but funding is “either… or…”
Some patient could benefit from both SGLT-2 inhibitor and GLP-1 agonists. If they are willing to self-fund, self-funding SGLT-2 inhibitor ($80-100/month) is cheaper than self-funding GLP-1 agonists ($150-250/month)
DPP-4 inhibitor (e.g. Vildagliptin / Galvus / Galvumet) would have to be ceased when GLP-1 agonist is initiated.
Weight loss
Available in NZ = Liraglutide high dose (Saxenda, daily injection)
Self-funding needed ($500-600/month)
Not available in NZ = Semaglutide (Ozempic, Wegovy) or Tirzepatide (Mounjaro), as of May 2023
Side effects, particularly upper gastrointestinal, are common with GLP-1 agonist initiation. Slow up-titration is usually advisable for Liraglutide (Saxenda).
Should patients see an endocrinologist?
GLP-1 agonist initiation could be done in primary care, as long as primary care doctor and team are comfortable.
Those who have complex or difficult-to-control diabetes, or those intending to use GLP-1 agonist for weight loss are encouraged to see an endocrinologist.
David Kim, endocrinologist