
Why is it important to know?
Venous disease affects all age groups, gender and racial groups
25% of the population has a degree of venous disease
If untreated it can progress all the way from visible varicosities to skin pigmentation and ultimately tissue loss/ ulceration
Prevalence of venous ulcers (VLUs) in NZ is in the order of 2.48 per 1000 adults.

Chronic venous insufficiency is incredibly common. Brand et al. Am J Prev Med 1988
Pathophysiology
Venous reflux develops when the valves stop working properly and allow blood to flow backward (i.e., reflux) and pool in the lower leg veins.
Risk factors include
age
family history
obesity
pregnancy
lack of exercise
leg injury or trauma
prolonged sitting or standing

Diseased valves cause blood to move in both directions, elevating venous pressure.

Focal dilation is typically asymptomatic, with little to no visual appearance. Varicosity and aneurysm are usually more symptomatic.
CEAP Classification

C = clinical; E = etiologic; A = anatomic; P = pathophysiologic
Who to refer?
Public
Thrombophlebitis
Skin change
Healed/ Open Venous Ulcer
Private (in addition)
moderately severe pain/ swelling not responsive to simple analgesics
episode of bleeding from a burst varicosity
Vein map
Femoral vein; saphenofemoral junction (SFJ), great saphenous vein (GSV)
Popliteal vein; small saphenous vein (SSV)
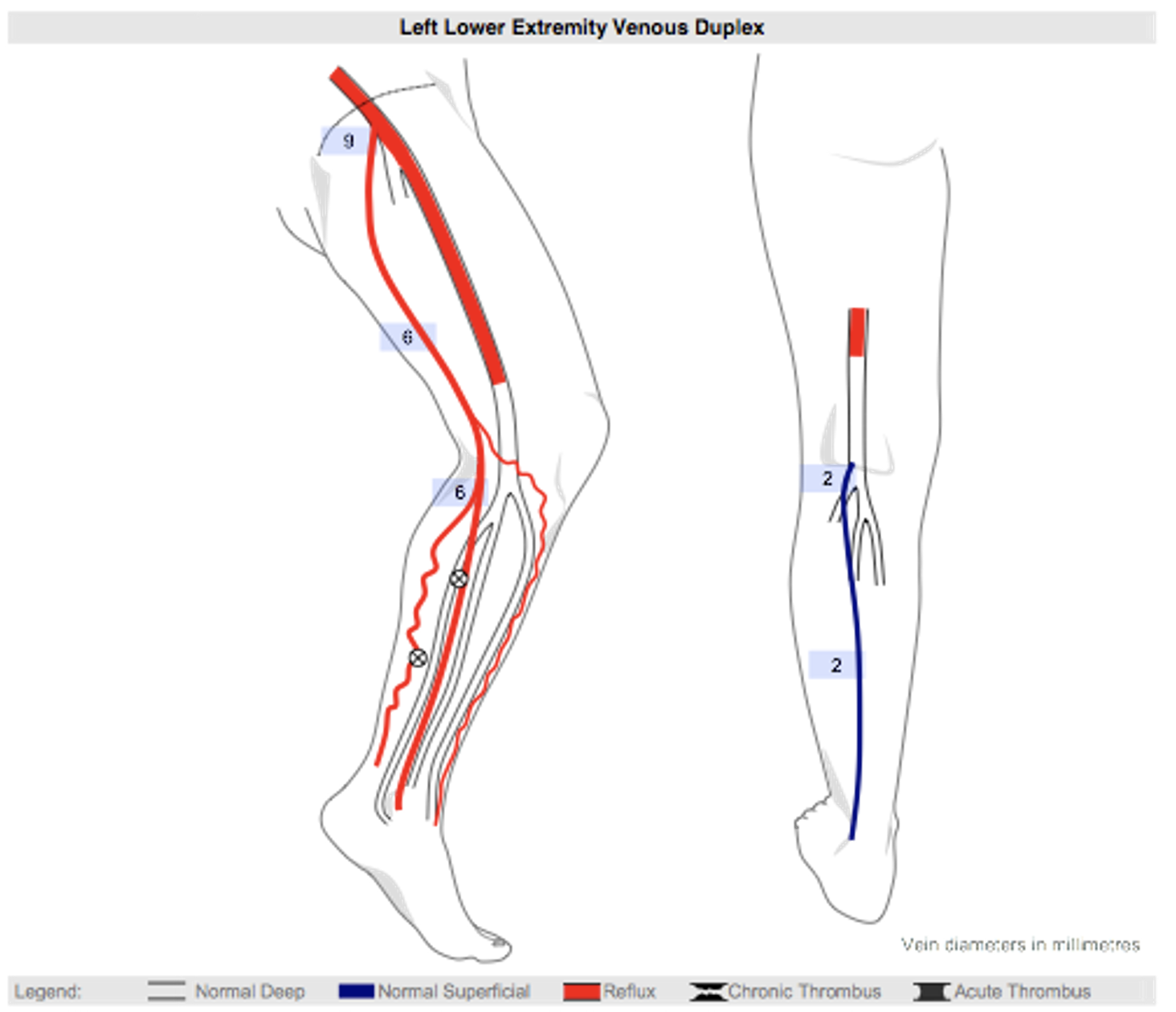
In this example, deep veins reflux to the level of the distal FV. POP vein and deep calf veins are competent. SPJ, GSV, and GSV tributaries in the calf reflux as shown. SPJ and SSV are competent. Two incompetent perforators were detected.
Treatment options
Conservative
Exercise
Elevation
Compression stockings
NSAIDS
Interventional
Surgical stripping
Thermal
Laser ablation
Radiofrequency ablation - for incompetent saphenous veins
Small access sheath placed into the saphenous vein
Through this the thin RFA probe is placed and manipulated to 2cm proximal to the SFJ/ SPJ
Non-thermal
Mechanochemical ablation
Foam Sclerotherapy - for small incompetent tributaries
Sodium Tetradecyl Sulphate is mixed with air to foam a foam an injected into the tributaries under ultrasound guidance
The foam displaces the blood in the vein and destroys the lining of the vein. The vein shuts down and is gradually broken down and absorbed
Cyanoacrylate ablation
Post-procedural care - RFA and sclerotherapy
Thigh high level II compression stocking for 10 days (helps with pain, swelling, prevent haematoma formation).
Analgesics, NSAIDs
Walking: keeps calves pumping blood through deep veins and helps prevent DVT (1% risk).
Follow up appointment in 6 weeks. Ultrasound the legs with further sclerotherapy if needed for residual tributaries
Dr Rahul Bera
