

There has been increasing evidence of rhythm control in AF. This is what we know in 2024:
Aim for rhythm control of AF in most patients
Earlier consideration of AF ablation, especially in those with heart failure (without alternative cause)
Rate-related and arrhythmia-related cardiomyopathy under-appreciated
<75y (up to 80y) for AF ablation
In those not suitable for rhythm control
If signs of HF or LV impaired, consider cardiac device and AV node ablation
Here is the evidence base:
AF with HF
Castle AF 2018 - Marrouche et al. NEJM. 2018
Sx paroxysmal or persistent, LVEF <35%, NYHA II
n=363
Death = 13.4% vs. 25%
Death or HF hospitalisation = 28.5% vs. 44.6%
CASTLE HTx 2023
AF wit hens stage HF, mean LVEF 25-29%
n=97
Primary (death, IVAD, transplant) = 8% vs. 30%
Death = 6% vs. 20%
LVEF improved by 6.7%
AF burden reduced by 31%
AF without HF
Cabana 2019
Sx, age>65 or age<65 with >1 stroke risk
Primary (death, disabling stroke, serious bleed, cardiac arrest) = non-significant
Hospitalisation reduced
AF burden reduced
Quality of life improved
EAST-AFNET 4 2020 - Kirchhof NEJM 2020
Recent AF, age>75, prior TIA/stroke,
OR 2 of age>65, female, HF, HT, DM, severe CAD, CKD, LVH
n=2789
Primary (death, stroke, HF hospitalisation, ACS) = 3.9% vs. 5.0%
Serious adverse events with rhythm medications = 4.9% vs. 1.4%
STOP-AF First 2020
Sx, paroxysmal
n=203
Treatment success @1y = 75% vs. 45%
CRYO-FIRST 2021 - Kuniss Europe 2021
Sx, paroxysmal
n=218
Free from AF @1y = 82% vs. 68%
EARLY-AF 2020 - Andrade NEJM 2020, 2023
Sx, paroxysmal
n=303
Free from AF recurrence = 57% vs. 32%
Persistent AF @ 3y = 1.9% vs. 7.4%
Median AF burden @ 3y = 0.00% vs. 0.24%
Serious adverse event @ 3y = 4.5% vs. 10.1%
This is the proposed algorithm
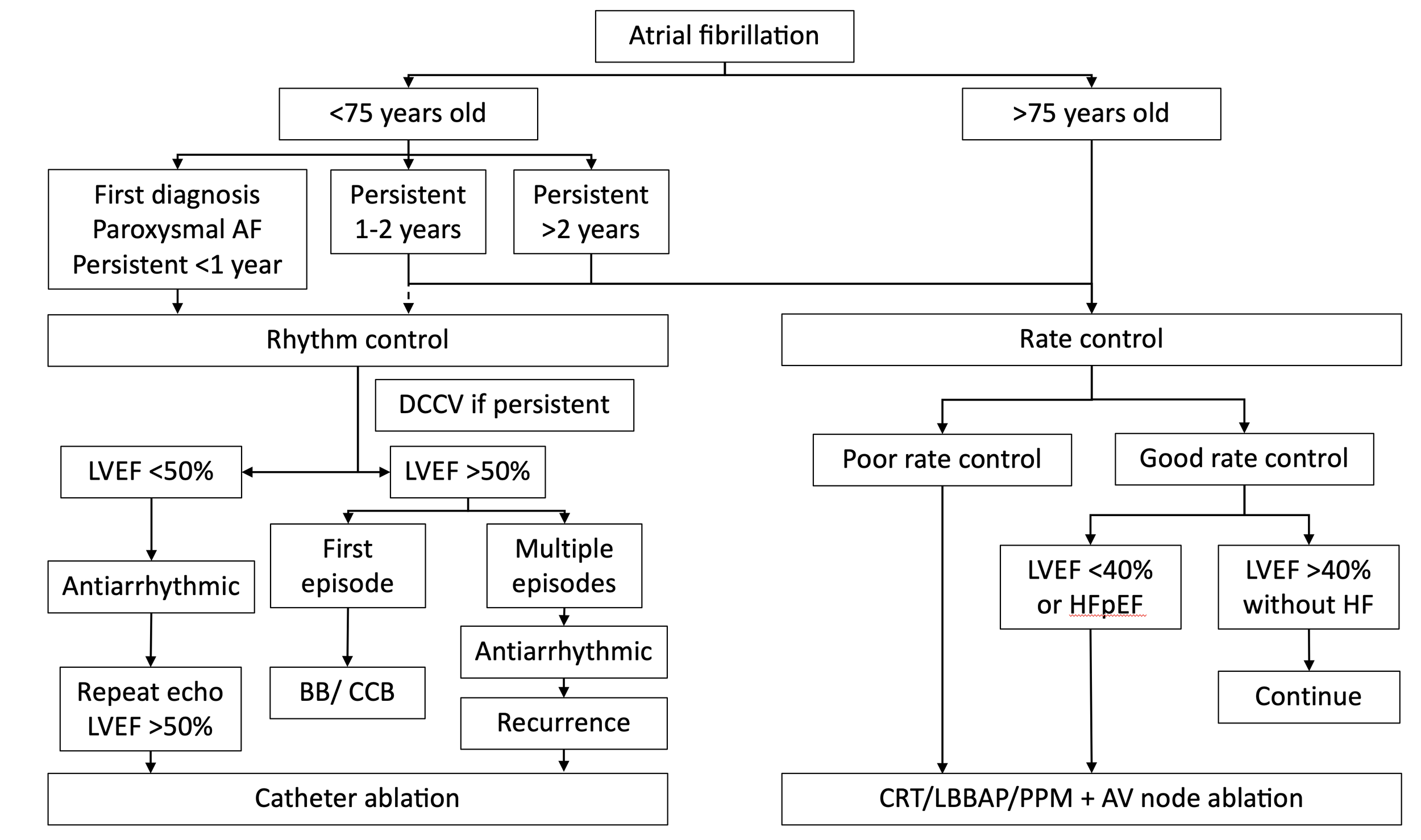
Conceptual algorithm of how we may pick rhythm control vs. rate control
Dr Shawn Foo