

ECG interpretation could be difficult, but a simplified approach would serve us well 95% of the time. Here is my approach:
Read moreNTproBNP - when should I actually order one?

BNP Synthesis; JACC 2016;68:22
NTproBNP is a very useful test in heart failure. However, often it is overused, as the diagnosis of heart failure should be a clinical one.
Here are the scenarios where it may be useful:
Hypertension treatment – how should we choose?

Billy Apple @ Auckland Art Gallery 2015 (2 Minutes 33 Seconds (Red))
First line agents for hypertension are one of three classes:
- ACE inhibitors or Angiotensin receptor blockers
- Thiazides
- Calcium channel blockers
Drug preference is mainly influenced by co-morbidities and contraindications, rather than a simple age cut-off.
Read moreBeta-blockers in Hypertension

70-year-old asymptomatic man with hypertension but not cardiovascular disease presented for a routine check. His pulse rate was 40bpm. His son, aged 45, recently had an MI in Australia.
His medications include
Doxazosin 8mg OD
Metoprolol 95mg CR OD – since 2006
Cilazapril 5mg / Hydrochlorothiazide 12.5mg OD
ECG shows sinus bradycardia, with normal PR interval, QRS duration.
Read moreBP therapy initiation - Combination vs. Single Agent

Expected BP lowering with different anti-hypertensive classes and dosages.
65M with Type 2 diabetes on oral hypoglycaemics but no proven coronary artery disease, BP 150/95mmHg despite 3 months of intensive lifestyle modifications, not currently on anti-hypertensives. Would you?
- Introduce low dose ACE inhibitors, with gradual up-titration
- Introduce combination ACE inhibitor / thiazide, with up-titration later on
Read moreEndocarditis prophylaxis

Enterococcus faecalis
Antibiotic prophylaxis is suggested for patients with cardiac conditions that confer the highest risk of adverse outcome from infective endocarditis.
Read moreMaking sense of an echocardiogram report - for GPs!
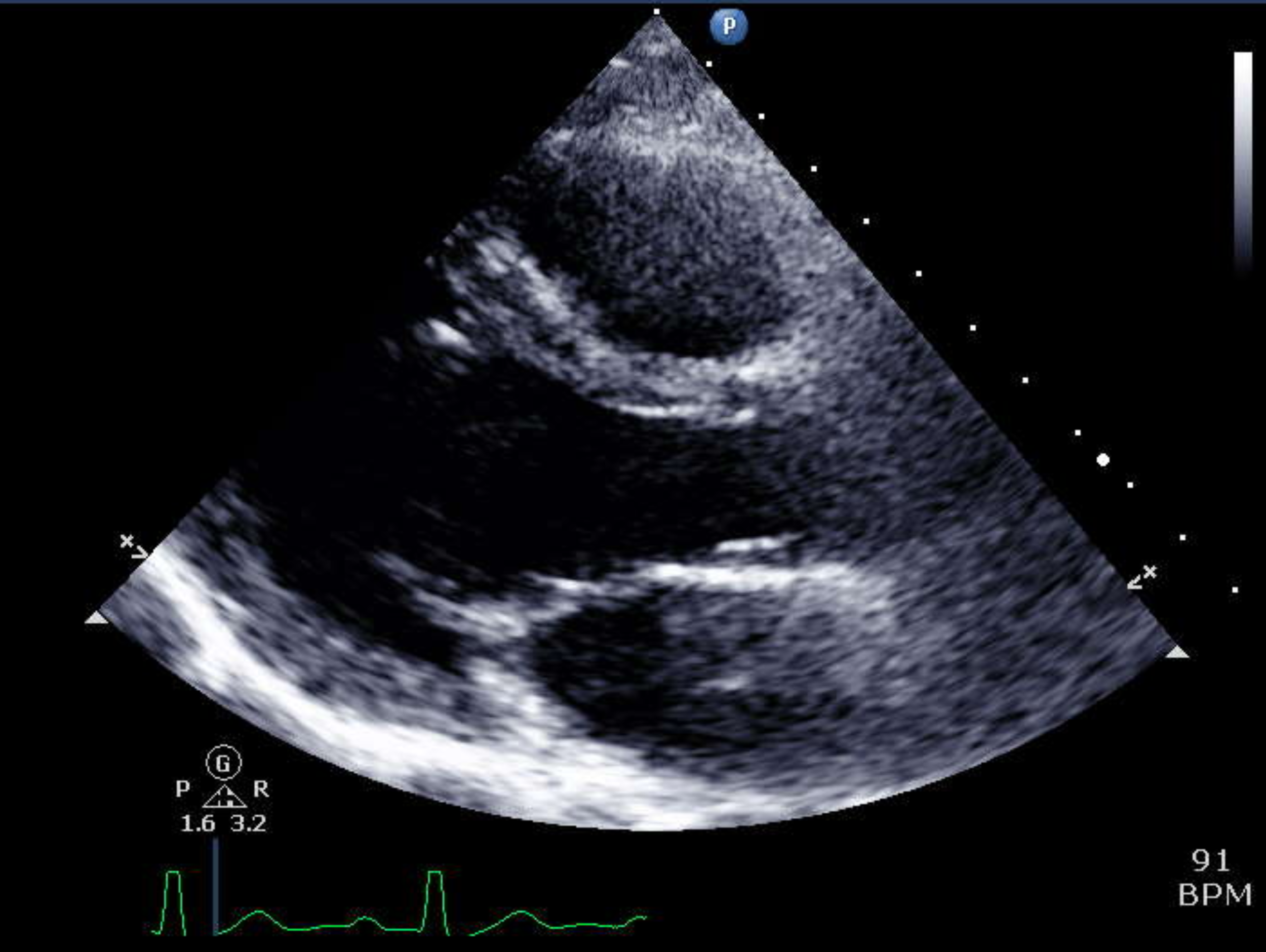
GPs often receive echocardiogram reports and are asked to interpret them. Here is a grossly simplified version of how.
Read moreFish oil supplement? - update 2018

Monterey Aquarium
Daily supplementation with marine-derived omega-3 fatty acids has been promoted for its potential health benefits in cardiovascular diseases. We blogged about this last year with a meta-analysis from Oxford. Here is the update.
The promised randomized controlled trial has now come out after the European Society of Cardiology Congress in Munich last week.
Read moreAlcohol consumption risk thresholds

See below!
Despite apparent “benefit” for heart attacks, increasing levels of alcohol consumption increase the risk of all-cause mortality and of cancers specifically, meaning that the level of consumption that minimises health loss is probably zero. At most, 100g per week is the absolute maximum before which risk increases significantly.
Read moreDuration of anti-platelets – a 2018 update

Cumulative Incidence of Major Adverse Cardiovascular and Cerebrovascular Events, According to Study Group. DAPT trial
64F presented with chest pain, consistent with non-ST elevation myocardial infarction with preserved systolic function. At invasive angiogram, right coronary artery was successfully stented with a drug eluting stent. On hospital discharge, she was given Aspirin, Ticagrelor as dual anti-platelet agents. How long should the dual antiplatelet therapy be continued for?
Read moreNocturnal hypertension

Arboria, 2015 @ Aotea Square
65M presented for a general health check, asymptomatic on systems enquiries. BP was 150/90mmHg with no other abnormalities. You decided to send him for an ambulatory blood pressure monitor to establish if more aggressive intervention is necessary. The report states that he is not a nocturnal dipper. His average diurnal BP was 145/85mmHg. Would medications be necessary? Is there anything else we should consider?
Read moreLifestyle changes for hypertension – exactly how effective is it?!

Topolobampo, Chicago, IL
In general practice (and in secondary care), we discuss at length lifestyle modifications that aid blood pressure lowering. But exactly how effective are the various strategies?
There are 5 things we could do to reduce our blood pressure, without medications.
Read moreAtrial fibrillation – is there a role for lifestyle modification?

Chocolate, camote, coconut @ Topolobampo, Chicago, IL
55M presented with first episode of paroxysmal atrial fibrillation proven on resting ECG in the GP practice. Echocardiogram showed structurally normal heart. The cardiologist decided to manage conservatively without starting anti-arrhythmics right now. Which of the following risk factor management should be part of his AF treatment and prevention?
Read moreACC AHA Hypertension Guidelines 2017 – What’s new?

@ AHA Meeting in Anaheim 2017 - taking notes
The ACC/AHA Hypertension Guidelines 2017 was released in the AHA meeting in Anaheim, Californiain November 2017.
While there were a lot of changes, I think it has simplified a lot of the complexities surrounding treatment threshold and goal.
Read more“My cholesterol is almost normal – why do I need statins, doctor?”

Baja hiramasa yellowtail, pineapple two ways, achiote infused agave @Topolobampo, Chicago, IL
Traditionally, we are taught that laboratory tests have “normal ranges”, such as in haemoglobin or creatinine. However, this concept of “normal”, when applied in cholesterol measurement, often creates confusion amongst some clinicians and certainly in most patients.
Read moreNSAIDs and MI risk

One-man-band on St Kilda Road, Melbourne
Nonsteroidal anti-inflammatory drugs (NSAIDs) use is associated with a significantly increased risk for myocardial infarction (MI). This includes naproxen, considered by some as one of the safest drugs in this class. This is according to a new patient level meta-analysis from the University of Montreal, studying celecopxib, diclofenac, ibuoprofen, naproxen and rofecoxib.
Read morePatient centered discussion of primary prevention statin therapy

Mayo clinic Statin Choice Decision Aid
The Mayo clinic has recently published an electronic tool called “Statin Choice Decision Aid”, which is immensely valuable in helping patients visualize cardiovascular risk, and the benefit of statin medications as applied to them.
Read moreECG Case 2016-09

32-year-old man presented with cough, breathlessness on exertion and interscapular pain. His ECG was as below.
- Reassure
- CXR, reassure
- CXR, take a more detailed history, then reassure
- CXR, full history, refer for further assessment
Read moreIndividual risk assessment - a common scenario

1906 San Francisco Fire Sacramento Street; Photo from Arnold Genthe from the Library of Congress
A 40-year-old Maori man came for routine review concerned because his 38-year-old brother, who was a smoker, died suddenly of a heart attack. The patient was athletic, previously played professional rugby, without clinical risk factors.
- BMI 28
- LDL 4.9; TC/HDL ratio 4
His calculated cardiovascular risk on these parameters was low. A reasonable approach would include
1) reinforcing healthy living and reassessing in 5 years
2) reinforcing healthy lifestyle and starting a statin
3) reinforcing healthy lifestyle, getting a CTCA, starting a statin
4) all of the above
Read moreAre cardiologists obsessed with statins?

Sam is a 60-year-old male heart attack survivor who had an unremarkable recovery after the successful coronary artery stenting in the middle of the night of his presentation. Now it is 3 months and Sam feels absolutely grand. At follow-up, his cardiologist insists that he should continue all the prescribed medications. He read on the internet some bad press about statin medications and thought, “surely, nothing will happen if I stop taking statins?!”
Read more